Exam 9: Section 3: Language and Thought
Exam 1: Section 1: Psychology: Evolution of a Science11 Questions
Exam 1: Section 2: Psychology: Evolution of a Science203 Questions
Exam 1: Section 3: Psychology: Evolution of a Science12 Questions
Exam 1: Section 4 : Psychology: Evolution of a Science108 Questions
Exam 1: Section 5: Psychology: Evolution of a Science16 Questions
Exam 1: Section 6 : Psychology: Evolution of a Science16 Questions
Exam 2: Section 1: Methods in Psychology16 Questions
Exam 2: Section 2: Methods in Psychology170 Questions
Exam 2: Section 3: Methods in Psychology12 Questions
Exam 2: Section 4: Methods in Psychology89 Questions
Exam 2: Section 5: Methods in Psychology16 Questions
Exam 2: Section 6: Methods in Psychology16 Questions
Exam 3: Section 1: Neuroscience and Behavior13 Questions
Exam 3: Section 2: Neuroscience and Behavior265 Questions
Exam 3: Section 3: Neuroscience and Behavior12 Questions
Exam 3: Section 4: Neuroscience and Behavior151 Questions
Exam 3: Section 5: Neuroscience and Behavior17 Questions
Exam 3: Section 6: Neuroscience and Behavior17 Questions
Exam 4: Section 1 : Sensation and Perception14 Questions
Exam 4: Section 2: Sensation and Perception246 Questions
Exam 4: Section 3: Sensation and Perception12 Questions
Exam 4: Section 4: Sensation and Perception151 Questions
Exam 4: Section 5: Sensation and Perception18 Questions
Exam 4: Section 6: Sensation and Perception17 Questions
Exam 5: Section 1: Consciousness12 Questions
Exam 5: Section 2: Consciousness229 Questions
Exam 5: Section 3: Consciousness13 Questions
Exam 5: Section 4: Consciousness116 Questions
Exam 5: Section 5: Consciousness15 Questions
Exam 5: Section 6: Consciousness16 Questions
Exam 6: Section 1: Memory12 Questions
Exam 6: Section 2: Memory239 Questions
Exam 6: Section 3: Memory11 Questions
Exam 6: Section 4: Memory123 Questions
Exam 6: Section 5: Memory16 Questions
Exam 6: Section 6: Memory15 Questions
Exam 7: Section 1: Learning15 Questions
Exam 7: Section 2: Learning210 Questions
Exam 7: Section 3: Learning13 Questions
Exam 7: Section 4: Learning154 Questions
Exam 7: Section 5 : Learning17 Questions
Exam 7: Section 6: Learning16 Questions
Exam 8: Section 1: Emotion and Motivation14 Questions
Exam 8: Section 2: Emotion and Motivation156 Questions
Exam 8: Section 3: Emotion and Motivation13 Questions
Exam 8: Section 4: Emotion and Motivation102 Questions
Exam 8: Section 5: Emotion and Motivation15 Questions
Exam 8: Section 6: Emotion and Motivation15 Questions
Exam 9: Section 1: Language and Thought11 Questions
Exam 9: Section 2: Language and Thought165 Questions
Exam 9: Section 3: Language and Thought13 Questions
Exam 9: Section 4: Language and Thought118 Questions
Exam 9: Section 5: Language and Thought15 Questions
Exam 9: Section 6: Language and Thought15 Questions
Exam 10: Section 1: Intelligence12 Questions
Exam 10: Section 2: Intelligence128 Questions
Exam 10: Section 3: Intelligence12 Questions
Exam 10: Section 4 : Intelligence92 Questions
Exam 10: Section 5: Intelligence15 Questions
Exam 10: Section 6 : Intelligence15 Questions
Exam 11: Section 1: Development13 Questions
Exam 11: Section 2: Development192 Questions
Exam 11: Section 3: Development14 Questions
Exam 11: Section 4: Development102 Questions
Exam 11: Section 5: Development15 Questions
Exam 11: Section 6: Development15 Questions
Exam 12: Section 1: Personality11 Questions
Exam 12: Section 2: Personality194 Questions
Exam 12: Section 3: Personality14 Questions
Exam 12: Section 4: Personality98 Questions
Exam 12: Section 5: Personality16 Questions
Exam 12: Section 6: Personality15 Questions
Exam 13: Section 1: Social Psychology12 Questions
Exam 13: Section 2: Social Psychology189 Questions
Exam 13: Section 3: Social Psychology16 Questions
Exam 13: Section 4: Social Psychology94 Questions
Exam 13: Section 5: Social Psychology14 Questions
Exam 13: Section 6: Social Psychology15 Questions
Exam 14: Section 1: Stress and Health12 Questions
Exam 14: Section 2: Stress and Health128 Questions
Exam 14: Section 3: Stress and Health13 Questions
Exam 14: Section 4: Stress and Health91 Questions
Exam 14: Section 5: Stress and Health15 Questions
Exam 14: Section 6: Stress and Health15 Questions
Exam 15: Section 1: Psychological Disorders9 Questions
Exam 15: Section 2: Psychological Disorders158 Questions
Exam 15: Section 3: Psychological Disorders12 Questions
Exam 15: Section 4: Psychological Disorders91 Questions
Exam 15: Section 5 : Psychological Disorders15 Questions
Exam 15: Section 6: Psychological Disorders15 Questions
Exam 16: Section1 : Treatment of Psychological Disorders12 Questions
Exam 16: Section 2: Treatment of Psychological Disorders164 Questions
Exam 16: Section 3: Treatment of Psychological Disorders12 Questions
Exam 16: Section 4: Treatment of Psychological Disorders99 Questions
Exam 16: Section 5: Treatment of Psychological Disorders14 Questions
Exam 16: Section 6: Treatment of Psychological Disorders15 Questions
Exam 17: Intelligence Testing and Psychological Perspectives173 Questions
Select questions type
Scenario II
Scenario II is based on and presents results consistent with the following study:
Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1997). Deciding advantageously before knowing the advantageous strategy. Science, 275(5304), 1293-1295. doi:10.1126/science.275.5304.1293
Bechara et al. (1997) studied risky decision making on a gambling task in patients with brain damage in an area critically involved in executive functions such as planning and decision making. They compared this performance with the performance of control participants without brain damage. All participants were given a starting bankroll of $2,000 in facsimile dollars. In the baseline condition, participants chose cards from among four decks. Selecting cards from Decks A and B sometimes resulted in a win of $100. Selecting cards from Decks C and D sometimes resulted in a win of $50. No losses were incurred in this condition. In the subsequent experimental condition, however, some cards in all decks produced losses. The losses in Decks A and B were large and occurred frequently enough to possibly result in bankruptcy. The losses in Decks C and D were considerably smaller. Bechara et al. measured deck selection and the galvanic skin response (GSR) both prior to (anticipatory) and after (post-outcome) turning over each card.
In the baseline condition, all participants in both groups showed a clear preference for Decks A and B. Both groups showed small but reliable anticipatory and post-outcome GSRs. In the experimental condition, with continued play the controls exhibited a clear preference for Decks C and D, while the patients continued to play more from Decks A and B. Relative to the baseline condition, controls exhibited a much larger anticipatory GSR prior to each decision whereas the patients' anticipatory GSR was small and similar to that obtained under the baseline condition. The post-outcome GSRs were similar in the two groups and occurred to both wins and losses.
Interestingly, the investigator systematically interrupted play during the experimental condition and asked all participants if they had developed a game strategy. With continued play, most of the control participants labeled Decks A and B as "the bad decks." Among the patients with brain damage, only half eventually labeled Decks A and B as "the bad decks." Remarkably, in both groups this realization did not affect game play. The minority of the control group who did not express a negative opinion about Decks A and B nevertheless tended to avoid those decks. Similarly, the patients who acknowledged that Decks C and D were risky nevertheless preferred those decks.
-(Scenario II) The results of this experiment suggest that the ability to correctly identify optimal game strategy is:
Free
(Multiple Choice)
4.9/5  (26)
(26)
Correct Answer: Verified
Verified
A
Scenario I
Scenario I is based on and presents results consistent with the following studies:
Snedeker, J., Geren, J., & Shafto, C. L. (2012). Disentangling the effects of cognitive development and linguistic expertise: A longitudinal study of the acquisition of English in internationally-adopted children. Cognitive Psychology, 65(1), 39-76. doi:10.1016/j.cogpsych.2012.01.004
Snedeker, J., Geren, J., & Shafto, C. L. (2007). Starting over: International adoption as a natural experiment in language development. Psychological Science, 18(1), 79-87. doi:10.1111/j.1467-9280.2007.01852.x
Language development occurs in orderly stages, beginning with one-word utterances and progressing to two-word utterances, simple sentences containing function morphemes, and the emergence of grammatical rules. Psycholinguists have attempted to determine if language development is a consequence of cognitive development or if it reflects linguistic processes that occur independently of general cognitive development. Studies on the acquisition of a second language in internationally adopted children have provided insight into this research question. In a series of studies, Snedeker et al. (2007, 2012) studied the acquisition of the English language in adopted preschoolers from China. These children had no exposure to the English language before being adopted by families in the United States.
Figure 9.1 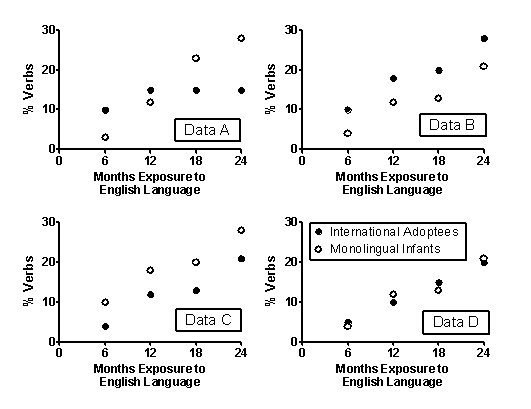 -(Scenario I) In a second study, Snedeker et al. (2012) found that older (e.g., 5 year-old) internationally adopted children acquiring English as a second language began correctly using words pertaining to time (e.g., yesterday, tomorrow) earlier in their exposure to English than monolingual infant controls. This observed difference is best interpreted as:
-(Scenario I) In a second study, Snedeker et al. (2012) found that older (e.g., 5 year-old) internationally adopted children acquiring English as a second language began correctly using words pertaining to time (e.g., yesterday, tomorrow) earlier in their exposure to English than monolingual infant controls. This observed difference is best interpreted as:
Free
(Multiple Choice)
4.9/5 (37)
Correct Answer:Verified
D
Scenario II
Scenario II is based on and presents results consistent with the following study:
Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1997). Deciding advantageously before knowing the advantageous strategy. Science, 275(5304), 1293-1295. doi:10.1126/science.275.5304.1293
Bechara et al. (1997) studied risky decision making on a gambling task in patients with brain damage in an area critically involved in executive functions such as planning and decision making. They compared this performance with the performance of control participants without brain damage. All participants were given a starting bankroll of $2,000 in facsimile dollars. In the baseline condition, participants chose cards from among four decks. Selecting cards from Decks A and B sometimes resulted in a win of $100. Selecting cards from Decks C and D sometimes resulted in a win of $50. No losses were incurred in this condition. In the subsequent experimental condition, however, some cards in all decks produced losses. The losses in Decks A and B were large and occurred frequently enough to possibly result in bankruptcy. The losses in Decks C and D were considerably smaller. Bechara et al. measured deck selection and the galvanic skin response (GSR) both prior to (anticipatory) and after (post-outcome) turning over each card.
In the baseline condition, all participants in both groups showed a clear preference for Decks A and B. Both groups showed small but reliable anticipatory and post-outcome GSRs. In the experimental condition, with continued play the controls exhibited a clear preference for Decks C and D, while the patients continued to play more from Decks A and B. Relative to the baseline condition, controls exhibited a much larger anticipatory GSR prior to each decision whereas the patients' anticipatory GSR was small and similar to that obtained under the baseline condition. The post-outcome GSRs were similar in the two groups and occurred to both wins and losses.
Interestingly, the investigator systematically interrupted play during the experimental condition and asked all participants if they had developed a game strategy. With continued play, most of the control participants labeled Decks A and B as "the bad decks." Among the patients with brain damage, only half eventually labeled Decks A and B as "the bad decks." Remarkably, in both groups this realization did not affect game play. The minority of the control group who did not express a negative opinion about Decks A and B nevertheless tended to avoid those decks. Similarly, the patients who acknowledged that Decks C and D were risky nevertheless preferred those decks.
-(Scenario II) The results of this experiment illustrate the role of emotional experience on decision making. Choice situations involving probabilistic outcomes often elicit feelings of anxiety, operationally defined in this study as:
Free
(Multiple Choice)
4.7/5 (36)
Correct Answer:Verified
A
Scenario I
Scenario I is based on and presents results consistent with the following studies:
Snedeker, J., Geren, J., & Shafto, C. L. (2012). Disentangling the effects of cognitive development and linguistic expertise: A longitudinal study of the acquisition of English in internationally-adopted children. Cognitive Psychology, 65(1), 39-76. doi:10.1016/j.cogpsych.2012.01.004
Snedeker, J., Geren, J., & Shafto, C. L. (2007). Starting over: International adoption as a natural experiment in language development. Psychological Science, 18(1), 79-87. doi:10.1111/j.1467-9280.2007.01852.x
Language development occurs in orderly stages, beginning with one-word utterances and progressing to two-word utterances, simple sentences containing function morphemes, and the emergence of grammatical rules. Psycholinguists have attempted to determine if language development is a consequence of cognitive development or if it reflects linguistic processes that occur independently of general cognitive development. Studies on the acquisition of a second language in internationally adopted children have provided insight into this research question. In a series of studies, Snedeker et al. (2007, 2012) studied the acquisition of the English language in adopted preschoolers from China. These children had no exposure to the English language before being adopted by families in the United States.
Figure 9.1
-(Scenario I) Snedeker et al. (2007) refers to their research program as a "natural experiment." However, for which reason is it NOT an example of a true experimental design?
(Multiple Choice)
4.8/5 (36)
Scenario II
Scenario II is based on and presents results consistent with the following study:
Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1997). Deciding advantageously before knowing the advantageous strategy. Science, 275(5304), 1293-1295. doi:10.1126/science.275.5304.1293
Bechara et al. (1997) studied risky decision making on a gambling task in patients with brain damage in an area critically involved in executive functions such as planning and decision making. They compared this performance with the performance of control participants without brain damage. All participants were given a starting bankroll of $2,000 in facsimile dollars. In the baseline condition, participants chose cards from among four decks. Selecting cards from Decks A and B sometimes resulted in a win of $100. Selecting cards from Decks C and D sometimes resulted in a win of $50. No losses were incurred in this condition. In the subsequent experimental condition, however, some cards in all decks produced losses. The losses in Decks A and B were large and occurred frequently enough to possibly result in bankruptcy. The losses in Decks C and D were considerably smaller. Bechara et al. measured deck selection and the galvanic skin response (GSR) both prior to (anticipatory) and after (post-outcome) turning over each card.
In the baseline condition, all participants in both groups showed a clear preference for Decks A and B. Both groups showed small but reliable anticipatory and post-outcome GSRs. In the experimental condition, with continued play the controls exhibited a clear preference for Decks C and D, while the patients continued to play more from Decks A and B. Relative to the baseline condition, controls exhibited a much larger anticipatory GSR prior to each decision whereas the patients' anticipatory GSR was small and similar to that obtained under the baseline condition. The post-outcome GSRs were similar in the two groups and occurred to both wins and losses.
Interestingly, the investigator systematically interrupted play during the experimental condition and asked all participants if they had developed a game strategy. With continued play, most of the control participants labeled Decks A and B as "the bad decks." Among the patients with brain damage, only half eventually labeled Decks A and B as "the bad decks." Remarkably, in both groups this realization did not affect game play. The minority of the control group who did not express a negative opinion about Decks A and B nevertheless tended to avoid those decks. Similarly, the patients who acknowledged that Decks C and D were risky nevertheless preferred those decks.
-(Scenario II) What can be accurately inferred from Scenario II?
(Multiple Choice)
4.8/5 (37)
Scenario I
Scenario I is based on and presents results consistent with the following studies:
Snedeker, J., Geren, J., & Shafto, C. L. (2012). Disentangling the effects of cognitive development and linguistic expertise: A longitudinal study of the acquisition of English in internationally-adopted children. Cognitive Psychology, 65(1), 39-76. doi:10.1016/j.cogpsych.2012.01.004
Snedeker, J., Geren, J., & Shafto, C. L. (2007). Starting over: International adoption as a natural experiment in language development. Psychological Science, 18(1), 79-87. doi:10.1111/j.1467-9280.2007.01852.x
Language development occurs in orderly stages, beginning with one-word utterances and progressing to two-word utterances, simple sentences containing function morphemes, and the emergence of grammatical rules. Psycholinguists have attempted to determine if language development is a consequence of cognitive development or if it reflects linguistic processes that occur independently of general cognitive development. Studies on the acquisition of a second language in internationally adopted children have provided insight into this research question. In a series of studies, Snedeker et al. (2007, 2012) studied the acquisition of the English language in adopted preschoolers from China. These children had no exposure to the English language before being adopted by families in the United States.
Figure 9.1
-(Scenario I) Which is the BEST reason why the research question posed in Scenario I could not be answered by studying infants' acquisition of the English language and comparing it to infants' acquisition of the Spanish language in American-born bilingual homes?
(Multiple Choice)
4.8/5 (38)
Scenario I
Scenario I is based on and presents results consistent with the following studies:
Snedeker, J., Geren, J., & Shafto, C. L. (2012). Disentangling the effects of cognitive development and linguistic expertise: A longitudinal study of the acquisition of English in internationally-adopted children. Cognitive Psychology, 65(1), 39-76. doi:10.1016/j.cogpsych.2012.01.004
Snedeker, J., Geren, J., & Shafto, C. L. (2007). Starting over: International adoption as a natural experiment in language development. Psychological Science, 18(1), 79-87. doi:10.1111/j.1467-9280.2007.01852.x
Language development occurs in orderly stages, beginning with one-word utterances and progressing to two-word utterances, simple sentences containing function morphemes, and the emergence of grammatical rules. Psycholinguists have attempted to determine if language development is a consequence of cognitive development or if it reflects linguistic processes that occur independently of general cognitive development. Studies on the acquisition of a second language in internationally adopted children have provided insight into this research question. In a series of studies, Snedeker et al. (2007, 2012) studied the acquisition of the English language in adopted preschoolers from China. These children had no exposure to the English language before being adopted by families in the United States.
Figure 9.1
-(Scenario I) Which data set in Figure 9.1 provides the most support for the contention that language development is critically dependent on experience with the language?
(Multiple Choice)
4.9/5 (25)
Scenario II
Scenario II is based on and presents results consistent with the following study:
Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1997). Deciding advantageously before knowing the advantageous strategy. Science, 275(5304), 1293-1295. doi:10.1126/science.275.5304.1293
Bechara et al. (1997) studied risky decision making on a gambling task in patients with brain damage in an area critically involved in executive functions such as planning and decision making. They compared this performance with the performance of control participants without brain damage. All participants were given a starting bankroll of $2,000 in facsimile dollars. In the baseline condition, participants chose cards from among four decks. Selecting cards from Decks A and B sometimes resulted in a win of $100. Selecting cards from Decks C and D sometimes resulted in a win of $50. No losses were incurred in this condition. In the subsequent experimental condition, however, some cards in all decks produced losses. The losses in Decks A and B were large and occurred frequently enough to possibly result in bankruptcy. The losses in Decks C and D were considerably smaller. Bechara et al. measured deck selection and the galvanic skin response (GSR) both prior to (anticipatory) and after (post-outcome) turning over each card.
In the baseline condition, all participants in both groups showed a clear preference for Decks A and B. Both groups showed small but reliable anticipatory and post-outcome GSRs. In the experimental condition, with continued play the controls exhibited a clear preference for Decks C and D, while the patients continued to play more from Decks A and B. Relative to the baseline condition, controls exhibited a much larger anticipatory GSR prior to each decision whereas the patients' anticipatory GSR was small and similar to that obtained under the baseline condition. The post-outcome GSRs were similar in the two groups and occurred to both wins and losses.
Interestingly, the investigator systematically interrupted play during the experimental condition and asked all participants if they had developed a game strategy. With continued play, most of the control participants labeled Decks A and B as "the bad decks." Among the patients with brain damage, only half eventually labeled Decks A and B as "the bad decks." Remarkably, in both groups this realization did not affect game play. The minority of the control group who did not express a negative opinion about Decks A and B nevertheless tended to avoid those decks. Similarly, the patients who acknowledged that Decks C and D were risky nevertheless preferred those decks.
-(Scenario II) Bechara et al. (1997) studied patients with brain damage in which of these areas?
(Multiple Choice)
4.9/5 (27)
Scenario I
Scenario I is based on and presents results consistent with the following studies:
Snedeker, J., Geren, J., & Shafto, C. L. (2012). Disentangling the effects of cognitive development and linguistic expertise: A longitudinal study of the acquisition of English in internationally-adopted children. Cognitive Psychology, 65(1), 39-76. doi:10.1016/j.cogpsych.2012.01.004
Snedeker, J., Geren, J., & Shafto, C. L. (2007). Starting over: International adoption as a natural experiment in language development. Psychological Science, 18(1), 79-87. doi:10.1111/j.1467-9280.2007.01852.x
Language development occurs in orderly stages, beginning with one-word utterances and progressing to two-word utterances, simple sentences containing function morphemes, and the emergence of grammatical rules. Psycholinguists have attempted to determine if language development is a consequence of cognitive development or if it reflects linguistic processes that occur independently of general cognitive development. Studies on the acquisition of a second language in internationally adopted children have provided insight into this research question. In a series of studies, Snedeker et al. (2007, 2012) studied the acquisition of the English language in adopted preschoolers from China. These children had no exposure to the English language before being adopted by families in the United States.
Figure 9.1
-(Scenario I) Which statement is an example of interpreting orderly changes in language development as a result of emerging cognitive skills?
(Multiple Choice)
4.8/5 (31)
Scenario I
Scenario I is based on and presents results consistent with the following studies:
Snedeker, J., Geren, J., & Shafto, C. L. (2012). Disentangling the effects of cognitive development and linguistic expertise: A longitudinal study of the acquisition of English in internationally-adopted children. Cognitive Psychology, 65(1), 39-76. doi:10.1016/j.cogpsych.2012.01.004
Snedeker, J., Geren, J., & Shafto, C. L. (2007). Starting over: International adoption as a natural experiment in language development. Psychological Science, 18(1), 79-87. doi:10.1111/j.1467-9280.2007.01852.x
Language development occurs in orderly stages, beginning with one-word utterances and progressing to two-word utterances, simple sentences containing function morphemes, and the emergence of grammatical rules. Psycholinguists have attempted to determine if language development is a consequence of cognitive development or if it reflects linguistic processes that occur independently of general cognitive development. Studies on the acquisition of a second language in internationally adopted children have provided insight into this research question. In a series of studies, Snedeker et al. (2007, 2012) studied the acquisition of the English language in adopted preschoolers from China. These children had no exposure to the English language before being adopted by families in the United States.
Figure 9.1
-(Scenario I) Figure 9.1 shows the number of verbs, expressed as a percentage of total English vocabulary, between 6 and 24 months of exposure to the English language in internationally adopted preschoolers from China and monolingual infants. Four fabricated sets of data (labeled A-D) are shown. Which data set provides the most support for the contention that cognitive factors play a role in language development?
(Multiple Choice)
4.8/5 (33)
Scenario I
Scenario I is based on and presents results consistent with the following studies:
Snedeker, J., Geren, J., & Shafto, C. L. (2012). Disentangling the effects of cognitive development and linguistic expertise: A longitudinal study of the acquisition of English in internationally-adopted children. Cognitive Psychology, 65(1), 39-76. doi:10.1016/j.cogpsych.2012.01.004
Snedeker, J., Geren, J., & Shafto, C. L. (2007). Starting over: International adoption as a natural experiment in language development. Psychological Science, 18(1), 79-87. doi:10.1111/j.1467-9280.2007.01852.x
Language development occurs in orderly stages, beginning with one-word utterances and progressing to two-word utterances, simple sentences containing function morphemes, and the emergence of grammatical rules. Psycholinguists have attempted to determine if language development is a consequence of cognitive development or if it reflects linguistic processes that occur independently of general cognitive development. Studies on the acquisition of a second language in internationally adopted children have provided insight into this research question. In a series of studies, Snedeker et al. (2007, 2012) studied the acquisition of the English language in adopted preschoolers from China. These children had no exposure to the English language before being adopted by families in the United States.
Figure 9.1
-(Scenario I) Snedeker et al. (2007) studied the acquisition of English as a second language in preschool children adopted from China. In trying to disentangle the role of linguistic and cognitive development on language acquisition, which of these would serve as the most appropriate control group?
(Multiple Choice)
4.9/5 (32)
Scenario II
Scenario II is based on and presents results consistent with the following study:
Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1997). Deciding advantageously before knowing the advantageous strategy. Science, 275(5304), 1293-1295. doi:10.1126/science.275.5304.1293
Bechara et al. (1997) studied risky decision making on a gambling task in patients with brain damage in an area critically involved in executive functions such as planning and decision making. They compared this performance with the performance of control participants without brain damage. All participants were given a starting bankroll of $2,000 in facsimile dollars. In the baseline condition, participants chose cards from among four decks. Selecting cards from Decks A and B sometimes resulted in a win of $100. Selecting cards from Decks C and D sometimes resulted in a win of $50. No losses were incurred in this condition. In the subsequent experimental condition, however, some cards in all decks produced losses. The losses in Decks A and B were large and occurred frequently enough to possibly result in bankruptcy. The losses in Decks C and D were considerably smaller. Bechara et al. measured deck selection and the galvanic skin response (GSR) both prior to (anticipatory) and after (post-outcome) turning over each card.
In the baseline condition, all participants in both groups showed a clear preference for Decks A and B. Both groups showed small but reliable anticipatory and post-outcome GSRs. In the experimental condition, with continued play the controls exhibited a clear preference for Decks C and D, while the patients continued to play more from Decks A and B. Relative to the baseline condition, controls exhibited a much larger anticipatory GSR prior to each decision whereas the patients' anticipatory GSR was small and similar to that obtained under the baseline condition. The post-outcome GSRs were similar in the two groups and occurred to both wins and losses.
Interestingly, the investigator systematically interrupted play during the experimental condition and asked all participants if they had developed a game strategy. With continued play, most of the control participants labeled Decks A and B as "the bad decks." Among the patients with brain damage, only half eventually labeled Decks A and B as "the bad decks." Remarkably, in both groups this realization did not affect game play. The minority of the control group who did not express a negative opinion about Decks A and B nevertheless tended to avoid those decks. Similarly, the patients who acknowledged that Decks C and D were risky nevertheless preferred those decks.
-(Scenario II) The results of this experiment suggest that individuals with this particular brain damage exhibit the greatest deficits in the ability to:
(Multiple Choice)
4.9/5 (29)
Scenario II
Scenario II is based on and presents results consistent with the following study:
Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1997). Deciding advantageously before knowing the advantageous strategy. Science, 275(5304), 1293-1295. doi:10.1126/science.275.5304.1293
Bechara et al. (1997) studied risky decision making on a gambling task in patients with brain damage in an area critically involved in executive functions such as planning and decision making. They compared this performance with the performance of control participants without brain damage. All participants were given a starting bankroll of $2,000 in facsimile dollars. In the baseline condition, participants chose cards from among four decks. Selecting cards from Decks A and B sometimes resulted in a win of $100. Selecting cards from Decks C and D sometimes resulted in a win of $50. No losses were incurred in this condition. In the subsequent experimental condition, however, some cards in all decks produced losses. The losses in Decks A and B were large and occurred frequently enough to possibly result in bankruptcy. The losses in Decks C and D were considerably smaller. Bechara et al. measured deck selection and the galvanic skin response (GSR) both prior to (anticipatory) and after (post-outcome) turning over each card.
In the baseline condition, all participants in both groups showed a clear preference for Decks A and B. Both groups showed small but reliable anticipatory and post-outcome GSRs. In the experimental condition, with continued play the controls exhibited a clear preference for Decks C and D, while the patients continued to play more from Decks A and B. Relative to the baseline condition, controls exhibited a much larger anticipatory GSR prior to each decision whereas the patients' anticipatory GSR was small and similar to that obtained under the baseline condition. The post-outcome GSRs were similar in the two groups and occurred to both wins and losses.
Interestingly, the investigator systematically interrupted play during the experimental condition and asked all participants if they had developed a game strategy. With continued play, most of the control participants labeled Decks A and B as "the bad decks." Among the patients with brain damage, only half eventually labeled Decks A and B as "the bad decks." Remarkably, in both groups this realization did not affect game play. The minority of the control group who did not express a negative opinion about Decks A and B nevertheless tended to avoid those decks. Similarly, the patients who acknowledged that Decks C and D were risky nevertheless preferred those decks.
-(Scenario II) Which of these was NOT a dependent variable?
(Multiple Choice)
4.8/5 (38)
Filters
- Essay(0)
- Multiple Choice(0)
- Short Answer(0)
- True False(0)
- Matching(0)